Fill Out a Valid Sports Physical Template
Guide to Writing Sports Physical
Filling out the Sports Physical form is an important step in ensuring that an athlete is ready for participation in sports activities. This form collects essential information about the athlete's health history and current medical status. To complete it accurately, follow the steps outlined below.
- Begin with the athlete's personal information: Write the athlete's name, gender, and date of birth at the top of the form.
- Fill in parent or guardian details: Include the names and daytime contact numbers for both the father and mother.
- Provide the athlete's address: Write the street address, city, state, and zip code.
- List an alternate emergency contact: Write the name and daytime phone number of an alternate contact person.
- Indicate any medical alerts: Note any allergies or specific medical conditions that the athlete has.
- Complete the medical history section: Answer each question regarding the athlete’s health history by marking 'YES,' 'NO,' or 'Don’t Know.' Be thorough and honest.
- Provide details for any 'YES' answers: If applicable, explain any 'YES' responses in the space provided.
- Leave the physical exam section for the physician: This section must be completed by a licensed medical professional during the physical examination.
- Physician's information: After the examination, the physician will fill in their name, address, and contact information.
- Signature and date: The physician will sign and date the form, certifying that the athlete is medically qualified to participate in sports.
- Participation restrictions: If there are any restrictions, the physician will note them in the designated area.
Document Breakdown
| Fact Name | Description |
|---|---|
| Purpose | The Sports Physical Form is designed to assess an athlete's health and fitness level to ensure they are safe to participate in sports activities. |
| Medical History | The form includes questions about the athlete's medical history, including family health issues and any past injuries. |
| Emergency Contacts | It requires the names and contact information for parents and an alternate emergency contact person. |
| Medical Alerts | Parents and athletes must indicate any medical alerts, such as allergies or chronic conditions, to inform healthcare providers. |
| Physical Examination | A licensed medical professional must complete the physical examination section, confirming the athlete's fitness for sports. |
| State-Specific Forms | Some states may have specific requirements or additional forms that must be completed in accordance with local laws. |
| Validity Period | Typically, a sports physical is valid for one year, after which a new examination is required. |
| Parental Consent | Parents or guardians must sign the form, indicating their consent for the athlete to participate in sports. |
| Confidentiality | The information provided on the Sports Physical Form is confidential and should only be shared with authorized personnel. |
FAQ
What is the purpose of the Sports Physical form?
The Sports Physical form is designed to assess an athlete's health and readiness for participation in sports. It collects important information about the athlete's medical history, current health status, and any potential risks. This form helps ensure that athletes are physically fit to compete and can help identify any health concerns that may need attention before they participate in sports activities.
Who needs to fill out the Sports Physical form?
All athletes participating in school sports or organized athletic programs typically need to complete the Sports Physical form. This includes students of all ages, from elementary through high school. Parents or guardians should assist younger athletes in filling out the form to ensure that all medical history and contact information is accurate and complete.
What kind of medical history information is required?
The form requires detailed medical history information, including:
- Family history of sudden death before age 50.
- Personal history of fainting, dizziness, or stopping exercise due to health issues.
- Any chronic illnesses or ongoing treatments.
- Allergies to medications or other substances.
- Past injuries, surgeries, or hospitalizations.
Providing complete and accurate information is crucial for the safety and health of the athlete.
What happens during the physical examination?
During the physical examination, a licensed medical professional will evaluate the athlete's overall health. This includes measuring height, weight, pulse, and blood pressure. The physician will also check various body systems such as eyes, ears, heart, lungs, and musculoskeletal health. The doctor will document any findings and determine if the athlete is medically qualified to participate in sports.
What should I do if the athlete has a medical condition?
If the athlete has a medical condition, it is essential to disclose this information on the Sports Physical form. The physician can provide guidance on how the condition may affect participation in sports. Depending on the situation, there may be recommendations for restrictions or additional evaluations. Open communication with the medical professional is key to ensuring the athlete's safety.
Fill out Other Forms
Hurt Feelings Report - The form reflects a commitment to humor in handling serious emotional matters.
The Check Register form is essential for effectively monitoring your financial activity, allowing both individuals and businesses to maintain a clear financial overview. To enhance your record-keeping, consider utilizing a Fillable Blank Check, which can aid in managing your transactions more efficiently and help prevent budgeting issues.
What Is W-3 - The W-3 plays a crucial role in connecting employer records with employee income data.
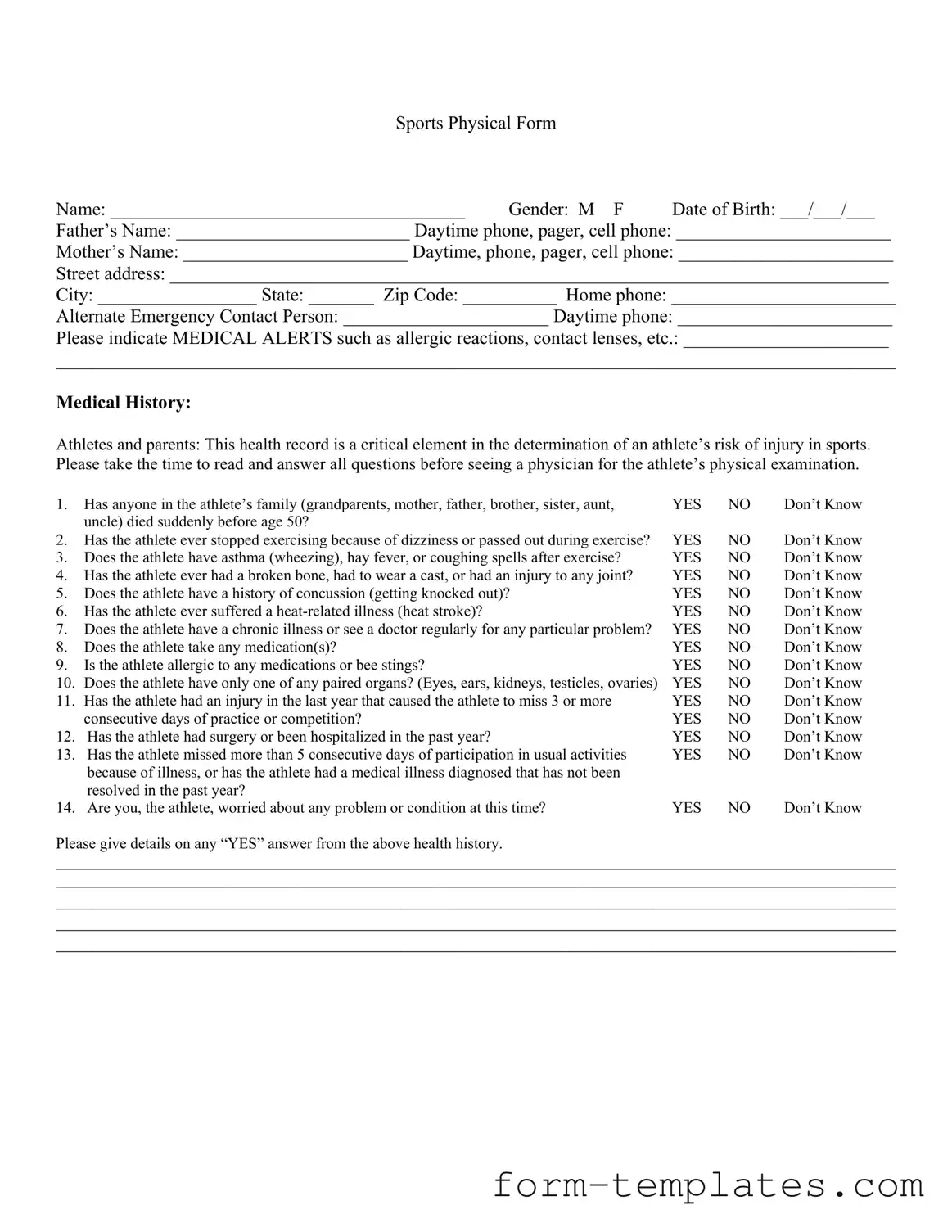
Sports Physical Example
Sports Physical Form
Name: ______________________________________ Gender: M F Date of Birth: ___/___/___
Father’s Name: _________________________ Daytime phone, pager, cell phone: _______________________
Mother’s Name: ________________________ Daytime, phone, pager, cell phone: _______________________
Street address: _____________________________________________________________________________
City: _________________ State: _______ Zip Code: __________ Home phone: ________________________
Alternate Emergency Contact Person: ______________________ Daytime phone: _______________________
Please indicate MEDICAL ALERTS such as allergic reactions, contact lenses, etc.: ______________________
__________________________________________________________________________________________
Medical History:
Athletes and parents: This health record is a critical element in the determination of an athlete’s risk of injury in sports. Please take the time to read and answer all questions before seeing a physician for the athlete’s physical examination.
1. |
Has anyone in the athlete’s family (grandparents, mother, father, brother, sister, aunt, |
YES |
NO |
Don’t Know |
|
uncle) died suddenly before age 50? |
|
|
|
2. |
Has the athlete ever stopped exercising because of dizziness or passed out during exercise? |
YES |
NO |
Don’t Know |
3. |
Does the athlete have asthma (wheezing), hay fever, or coughing spells after exercise? |
YES |
NO |
Don’t Know |
4. |
Has the athlete ever had a broken bone, had to wear a cast, or had an injury to any joint? |
YES |
NO |
Don’t Know |
5. |
Does the athlete have a history of concussion (getting knocked out)? |
YES |
NO |
Don’t Know |
6. |
Has the athlete ever suffered a |
YES |
NO |
Don’t Know |
7. |
Does the athlete have a chronic illness or see a doctor regularly for any particular problem? |
YES |
NO |
Don’t Know |
8. |
Does the athlete take any medication(s)? |
YES |
NO |
Don’t Know |
9. |
Is the athlete allergic to any medications or bee stings? |
YES |
NO |
Don’t Know |
10. |
Does the athlete have only one of any paired organs? (Eyes, ears, kidneys, testicles, ovaries) |
YES |
NO |
Don’t Know |
11. |
Has the athlete had an injury in the last year that caused the athlete to miss 3 or more |
YES |
NO |
Don’t Know |
|
consecutive days of practice or competition? |
YES |
NO |
Don’t Know |
12. Has the athlete had surgery or been hospitalized in the past year? |
YES |
NO |
Don’t Know |
|
13. Has the athlete missed more than 5 consecutive days of participation in usual activities |
YES |
NO |
Don’t Know |
|
|
because of illness, or has the athlete had a medical illness diagnosed that has not been |
|
|
|
|
resolved in the past year? |
|
|
|
14. |
Are you, the athlete, worried about any problem or condition at this time? |
YES |
NO |
Don’t Know |
Please give details on any “YES” answer from the above health history.
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
PHYSICAL EXAM – TO BE COMPLETED BY PHYSICIAN
Height __________ |
Weight __________ |
Pulse __________ |
Blood Pressure __________ |
Vision: R _____ / _____ uncorrected R _____ / _____ corrected |
L _____ / _____ uncorrected L _____ / _____ corrected |
||
Normal |
Abnormal Findings |
1.Eyes
2.Ears, Nose, Throat
3.Mouth & Teeth
4.Neck
5.Cardiovascular
6.Chest & Lungs
7.Abdomen
8.Skin
9.
10.Muskuloskeletal: ROM, strength, etc.
a.neck
b.spine
c.shoulders
d.arms/ hands
e.hips
f.thighs
g.knees
h.ankles
i.feet
11.Neuromuscular
Initials
Please Print/ Stamp
Physician’s Name ___________________________________________________________________________________
Street Address _____________________________________________________________________________________
City, State, Zip Code ________________________________________________________________________________
Telephone _________________________________________________________________________________________
I certify that I have examined this athlete and found him/her medically qualified to participate in sports. I also certify that I am a licensed medical physician, physician’s assistant, or family nurse practitioner. (Doctor of Chiropractic Medicine is not satisfactory.)
Physician Signature __________________________________________________________ Date __________________
PARTICIPATION RESTRICTIONS: _________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________