Fill Out a Valid Immunization Record Template
Guide to Writing Immunization Record
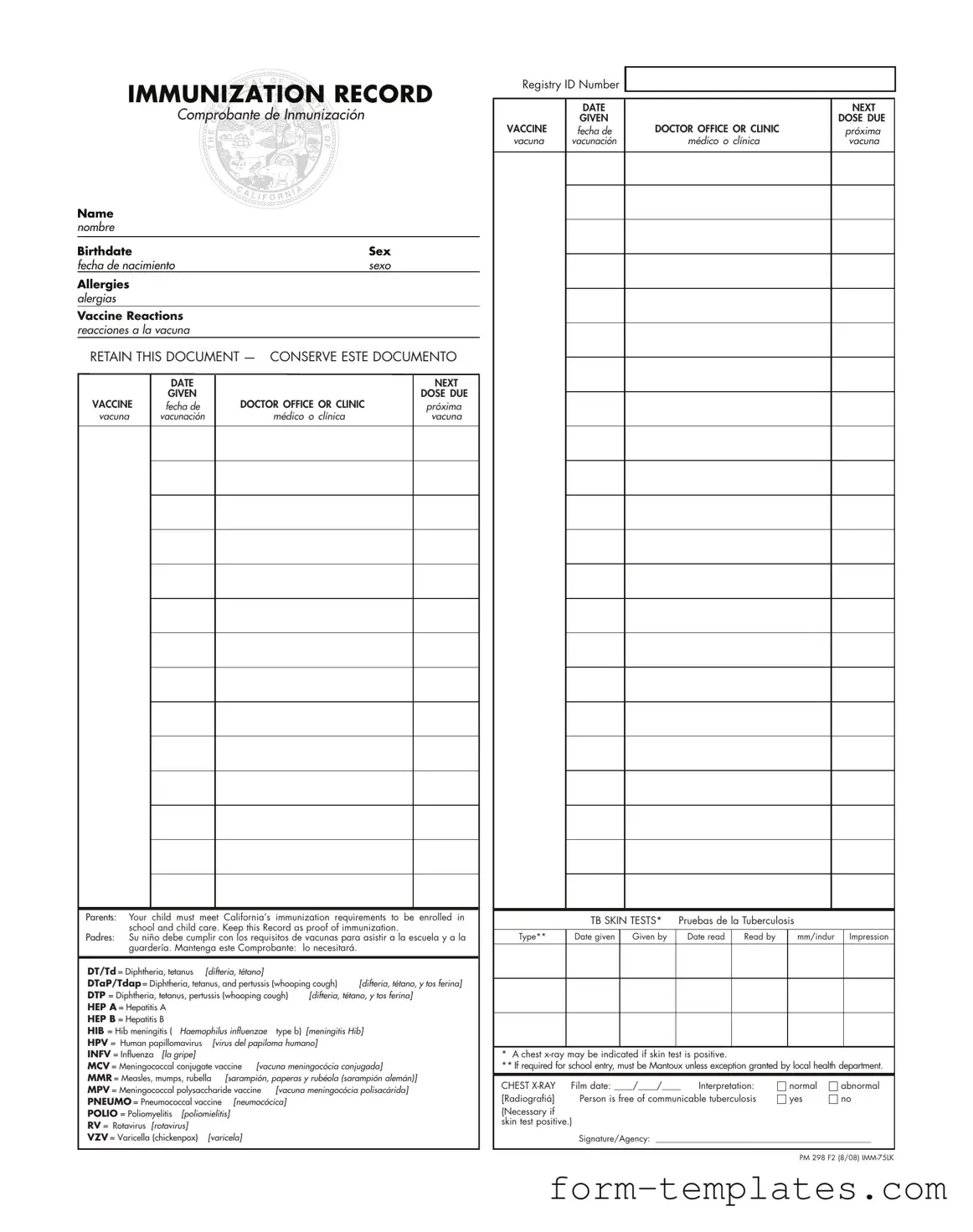
Completing the Immunization Record form is essential for maintaining accurate vaccination documentation. This record is necessary for school enrollment and child care in California. Follow the steps below to ensure that all required information is filled out correctly.
- Begin by entering the child's Name in the designated field.
- Fill in the Birthdate of the child.
- Indicate the child's Sex in the corresponding section.
- List any known Allergies the child may have.
- Document any Vaccine Reactions the child has experienced.
- Record the DATE NEXT GIVEN for the upcoming vaccine.
- Specify the DOSE DUE for the vaccine.
- Write down the name of the VACCINE being administered.
- Provide the name of the DOCTOR OFFICE OR CLINIC where the vaccine will be given.
- For the TB SKIN TESTS, indicate the type of test.
- Fill in the Date given and who administered the test.
- Record the Date read and the individual who read the results.
- Document the measurement in mm/indur and the impression of the test.
- If applicable, note the Film date for the chest x-ray.
- Indicate whether the interpretation was normal or abnormal.
- Finally, confirm if the person is free of communicable tuberculosis by marking yes or no.
- Sign the form and include the Agency name if applicable.
Document Breakdown
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Immunization Record form serves as proof of a child's immunizations, which is required for school and child care enrollment in California. |
| Required Vaccines | California law mandates that children receive specific vaccinations, including DTaP, MMR, and polio, among others, before attending school. |
| Allergy Information | Parents must disclose any allergies their child has, as this information is crucial for ensuring safe vaccination practices. |
| Vaccine Reactions | The form includes a section for documenting any adverse reactions to vaccines, helping healthcare providers monitor safety. |
| Retention of Document | It is important for parents to keep this document safe, as it may be needed for school enrollment and other health-related purposes. |
| TB Skin Tests | If required, TB skin tests must be conducted, and the results documented on the form to ensure compliance with health regulations. |
| Registry ID Number | A Registry ID Number is often included to track immunization records within the state's health system. |
| Signature Requirement | The form must be signed by a healthcare provider or agency, verifying that the information provided is accurate and complete. |
FAQ
What is the purpose of the Immunization Record form?
The Immunization Record form serves as an official document that tracks a child's vaccination history. It is essential for school enrollment and childcare in California. Parents must present this record to prove that their child has met the state's immunization requirements.
What information is included on the Immunization Record form?
The form contains various key details, including:
- Child's name and birthdate
- Sex of the child
- Allergies, if any
- Vaccine reactions
- Dates of vaccinations and upcoming doses
- Doctor's office or clinic information
This comprehensive information ensures that parents and healthcare providers have a clear record of immunizations administered.
Why is it important to keep this document?
Retaining the Immunization Record is crucial. Schools and childcare facilities require proof of immunizations for enrollment. If the record is lost, parents may face challenges in enrolling their child or may need to go through the process of obtaining replacement records from healthcare providers.
What vaccines are typically listed on the form?
The form includes a variety of vaccines, such as:
- Diphtheria, Tetanus, and Pertussis (DTaP/Tdap)
- Hepatitis A and B (HEP A, HEP B)
- Hib Meningitis (HIB)
- Human Papillomavirus (HPV)
- Influenza (INFV)
- Meningococcal Vaccines (MCV, MPV)
- Measles, Mumps, and Rubella (MMR)
- Pneumococcal (PNEUMO)
- Polio (POLIO)
- Rotavirus (RV)
- Varicella (VZV)
These vaccines protect against various infectious diseases and are critical for public health.
What should I do if my child has allergies or vaccine reactions?
If your child has known allergies or has experienced reactions to vaccines, it is important to document this information on the form. Discuss any concerns with your healthcare provider before administering new vaccines. They can provide guidance on safe vaccination practices tailored to your child's health needs.
What if my child needs a TB skin test?
If a TB skin test is required for school entry, it must be the Mantoux test unless an exception is granted by the local health department. The results of the test, including the date given and read, should be recorded on the Immunization Record. If the skin test is positive, a chest x-ray may be necessary to confirm the absence of communicable tuberculosis.
How can I obtain a replacement Immunization Record?
If the Immunization Record is lost, parents can contact their child's healthcare provider or the clinic where the vaccinations were administered. Many providers keep electronic records that can be accessed easily. Additionally, local health departments may also assist in providing a copy of immunization records.
Fill out Other Forms
Printable Truck Driver Daily Time Sheet - Creating a good driving record helps manage logistics more efficiently.
When dealing with a marital separation, understanding the importance of a well-drafted document is vital. Our guide covers various aspects of the Marital Separation Agreement you may need to consider. For further details, you can visit the important Marital Separation Agreement resources to help in the process.
Medicare and Social Security - Completing the CMS-1763 is a proactive way to manage Medicare responsibilities.
Immunization Record Example
IMMUNIZATION RECORD
Comprobante de Inmunización
Name nombre
Birthdate |
|
|
Sex |
||
fecha de nacimiento |
|
sexo |
|||
Allergies |
|
|
|
|
|
alergias |
|
|
|
|
|
Vaccine Reactions |
|
|
|
|
|
reacciones a la vacuna |
|
|
|
|
|
RETAIN THIS DOCUMENT — CONSERVE ESTE DOCUMENTO |
|||||
|
DATE |
|
|
NEXT |
|
|
|
|
|||
|
GIVEN |
|
|
DOSE DUE |
|
VACCINE |
fecha de |
DOCTOR OFFICE OR CLINIC |
|
próxima |
|
vacuna |
vacunación |
médico o clínica |
|
vacuna |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parents: Your child must meet California’s immunization requirements to be enrolled in school and child care. Keep this Record as proof of immunization.
Padres: Su niño debe cumplir con los requisitos de vacunas para asistir a la escuela y a la guardería. Mantenga este Comprobante: lo necesitará.
DT/Td = Diphtheria, tetanus |
[difteria, tétano] |
|
|
|
|
DTaP/Tdap = Diphtheria, tetanus, and pertussis (whooping cough) |
[difteria, tétano, y tos ferina] |
||||
DTP = Diphtheria, tetanus, pertussis (whooping cough) |
[difteria, tétano, y tos ferina] |
||||
HEP A = Hepatitis A |
|
|
|
|
|
HEP B = Hepatitis B |
|
|
|
|
|
HIB = Hib meningitis ( |
Haemophilus influenzae |
type b) |
[meningitis Hib] |
||
HPV = Human papillomavirus |
[virus del papiloma humano] |
|
|||
INFV = Influenza [la gripe] |
|
|
|
|
|
MCV = Meningococcal conjugate vaccine [vacuna meningocócia conjugada] |
|||||
MMR = Measles, mumps, rubella [sarampión, paperas y rubéola (sarampión alemán)] |
|||||
MPV = Meningococcal polysaccharide vaccine |
[vacuna meningocócia polisacárida] |
||||
PNEUMO = Pneumococcal vaccine [neumocócica] |
|
|
|||
POLIO = Poliomyelitis |
[poliomielitis] |
|
|
|
|
RV = Rotavirus [rotavirus] |
|
|
|
|
|
VZV = Varicella (chickenpox) |
[varicela] |
|
|
|
|
Registry ID Number
|
DATE |
|
NEXT |
|
GIVEN |
|
DOSE DUE |
VACCINE |
fecha de |
DOCTOR OFFICE OR CLINIC |
próxima |
vacuna |
vacunación |
médico o clínica |
vacuna |
|
TB SKIN TESTS* |
Pruebas de la Tuberculosis |
|
|
|||
|
|
|
|
|
|
|
|
Type** |
Date given |
Given by |
Date read |
Read by |
|
mm/indur |
Impression |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* A chest
** If required for school entry, must be Mantoux unless exception granted by local health department.
CHEST |
Film date: ____/____/____ |
Interpretation: |
|
normal |
|
abnormal |
|
[Radiografiá] |
Person is free of communicable tuberculosis |
|
yes |
|
|
no |
|
|
|
|
|||||
(Necessary if skin test positive.)
Signature/Agency: __________________________________________________
PM 298 F2 (8/08)