Fill Out a Valid DD 2870 Template
Guide to Writing DD 2870
Filling out the DD 2870 form is a straightforward process that requires careful attention to detail. Once you have completed the form, it will be submitted to the appropriate authority for processing. Make sure to review your entries for accuracy before sending it off.
- Begin by downloading the DD 2870 form from the official military website or obtaining a hard copy from your local military office.
- At the top of the form, fill in your personal information, including your full name, Social Security number, and contact details.
- In the designated section, indicate your relationship to the service member or veteran.
- Provide the service member's information, including their name, Social Security number, and branch of service.
- Carefully read the instructions on the form and ensure you understand each section before proceeding.
- Complete the required sections by providing any necessary details, such as the type of benefits or services you are requesting.
- If applicable, sign and date the form at the bottom to certify that all information is accurate and complete.
- Make a copy of the completed form for your records before submission.
- Submit the form according to the instructions provided, whether by mail or in person.
Document Breakdown
| Fact Name | Description |
|---|---|
| Purpose | The DD Form 2870 is used to authorize the release of medical information from military medical facilities. |
| Who Uses It | Service members, veterans, and their authorized representatives typically use this form to request access to medical records. |
| Submission Process | The completed form must be submitted to the appropriate military medical facility for processing. |
| Privacy Considerations | This form is governed by the Health Insurance Portability and Accountability Act (HIPAA), ensuring that personal health information is protected. |
| Validity | Once signed, the authorization remains valid until the individual revokes it or a specified expiration date is reached. |
FAQ
- Your full name and contact information
- The name of the individual or organization authorized to receive your records
- The specific information you wish to disclose
- The purpose of the disclosure
- Your signature and date
What is the DD 2870 form?
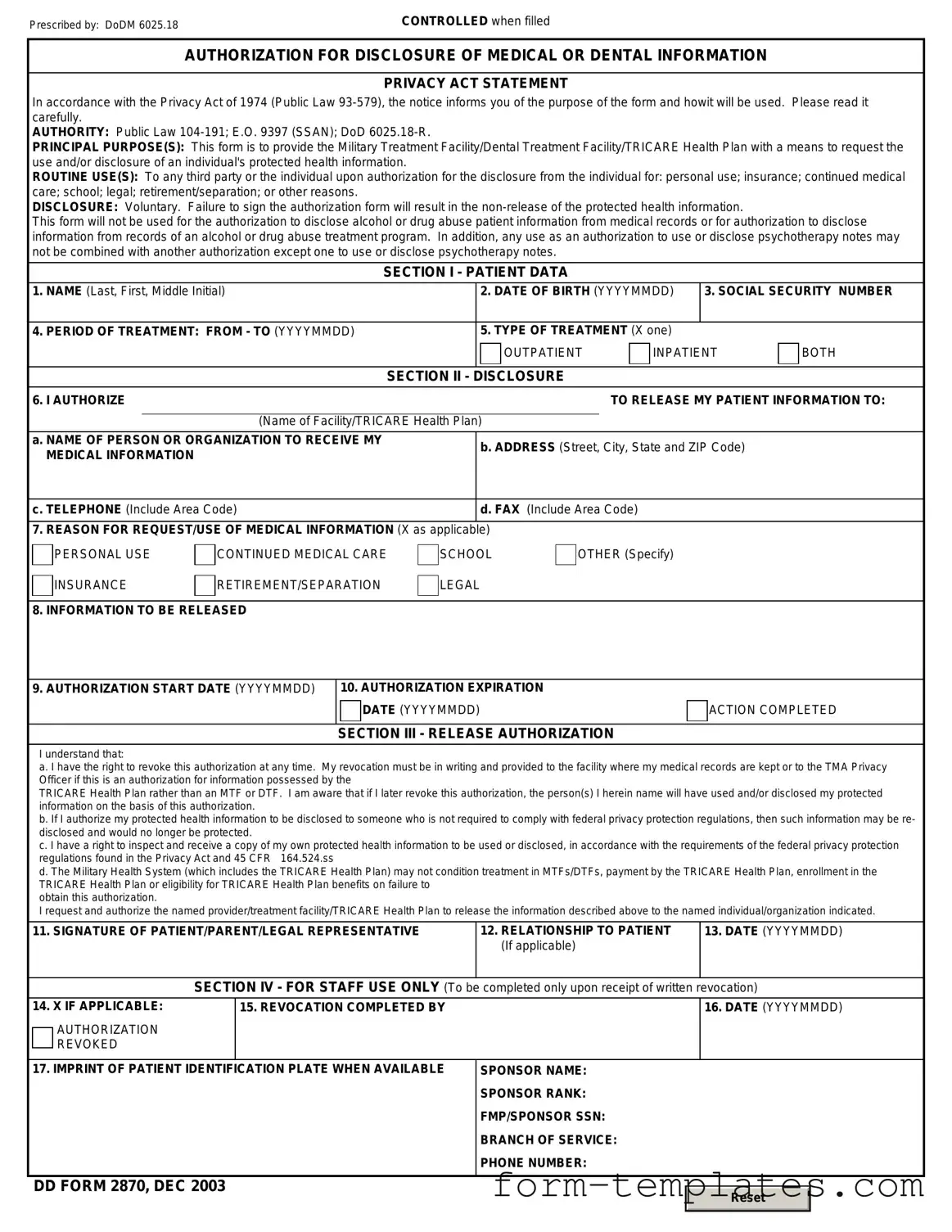
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is a document used by military personnel and their dependents. It allows individuals to authorize the release of their medical or dental records to specified parties. This form is crucial for ensuring that healthcare providers have the necessary permissions to share sensitive information.
Who needs to fill out the DD 2870 form?
Anyone who wishes to authorize the release of their medical or dental records must complete the DD 2870 form. This includes active duty service members, retirees, and eligible family members who require access to their medical information for various purposes, such as seeking treatment or filing claims.
How do I obtain a DD 2870 form?
You can obtain the DD 2870 form from several sources. It is available online through the official Department of Defense (DoD) website, military healthcare facilities, and other related organizations. Additionally, you may request a copy directly from your healthcare provider.
What information is required on the DD 2870 form?
When filling out the DD 2870 form, you will need to provide several key pieces of information, including:
How long is the DD 2870 form valid?
The validity of the DD 2870 form typically depends on the purpose of the disclosure. Generally, the authorization remains in effect until the purpose is fulfilled or until you revoke it in writing. It is advisable to check with the receiving party for their specific policies regarding expiration.
Can I revoke my authorization after submitting the DD 2870 form?
Yes, you can revoke your authorization at any time. To do so, you should submit a written notice to the party to whom you authorized the disclosure. Make sure to include your name, the date of the original authorization, and a statement that you wish to revoke it. This ensures that no further disclosures occur without your consent.
What should I do if my DD 2870 form is denied?
If your request for disclosure is denied, you should receive a written explanation outlining the reasons for the denial. If you believe the denial is unjust, you can request a review or appeal the decision. Be sure to follow the procedures outlined in the denial notice for the best chance of resolution.
Is there a fee associated with processing the DD 2870 form?
Typically, there is no fee for completing or submitting the DD 2870 form. However, some healthcare providers may charge for copying or sending medical records. It’s a good idea to check with the specific provider to understand any potential costs involved.
Where do I send the completed DD 2870 form?
After completing the DD 2870 form, you should send it to the healthcare provider or organization you wish to authorize for disclosure. Ensure you have the correct mailing address or contact information to avoid any delays in processing your request.
Can I fill out the DD 2870 form electronically?
Yes, many healthcare providers accept electronically signed DD 2870 forms. However, it's essential to check with the specific organization to ensure they accept electronic submissions. If they do, you may be able to complete the form online and submit it via email or a secure portal.
Fill out Other Forms
Erc Forms - Incorporates local market conditions and comparable sales data.
To ensure that you have the right tools for legal delegation, consider the importance of a practical General Power of Attorney form for handling your affairs efficiently. You can explore how this form works by visiting our guide on the critical aspects of General Power of Attorney.
Puppy Health Guarantee Template - The sales contract is binding and must be adhered to by both parties.
DD 2870 Example
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|