Fill Out a Valid Cna Shower Sheets Template
Guide to Writing Cna Shower Sheets
Filling out the CNA Shower Sheets form is an important process that helps ensure proper monitoring of a resident’s skin condition during showers. By following these steps, you can accurately document any abnormalities observed and communicate them effectively to the appropriate nursing staff.
- Start by writing the resident's name in the designated space labeled RESIDENT:.
- Next, enter the date of the assessment in the space labeled DATE:.
- Perform a visual assessment of the resident’s skin while giving the shower. Look for any abnormalities such as bruising, skin tears, or rashes.
- In the section titled Visual Assessment, check off any abnormalities that you observe from the provided list. If you notice something that is not listed, write it in the Other: section.
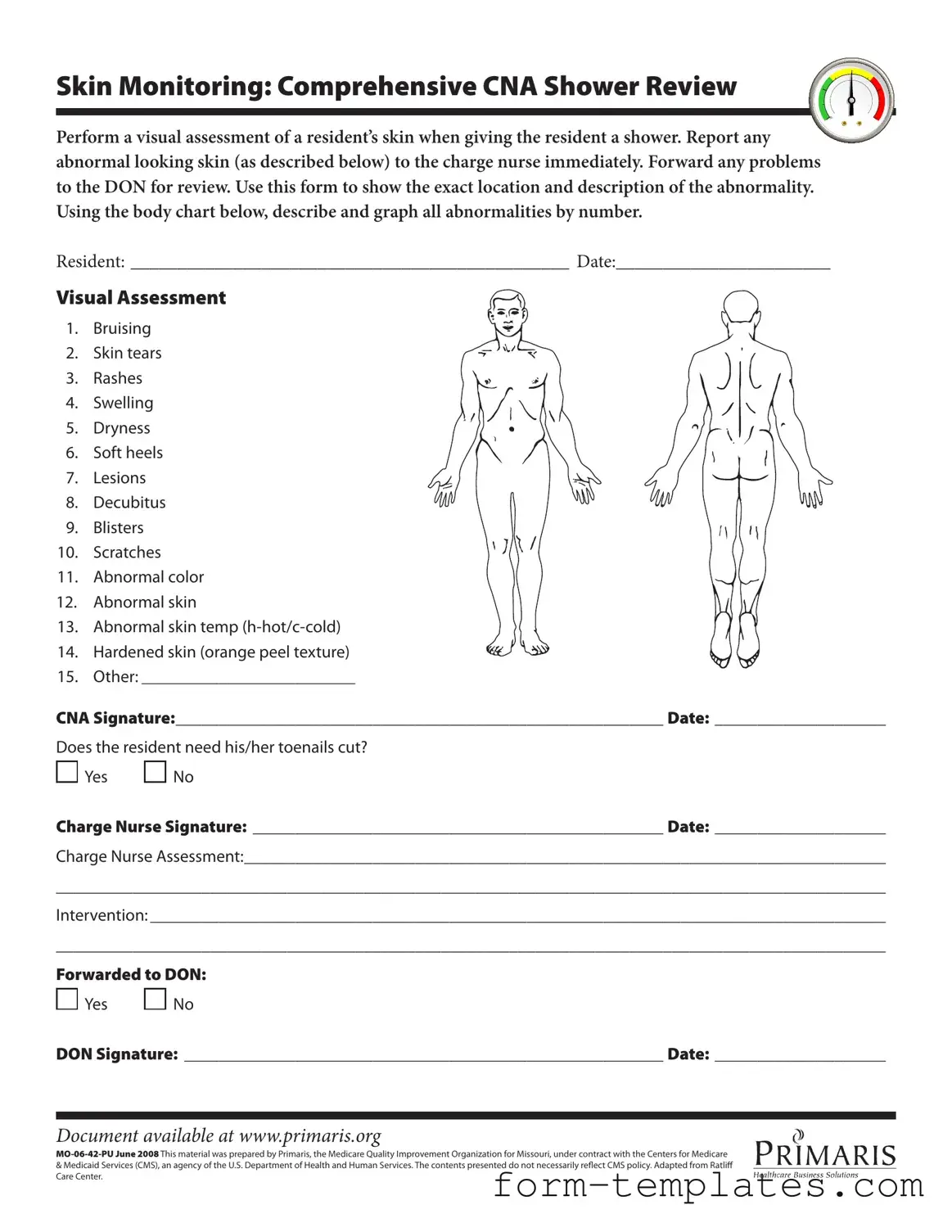
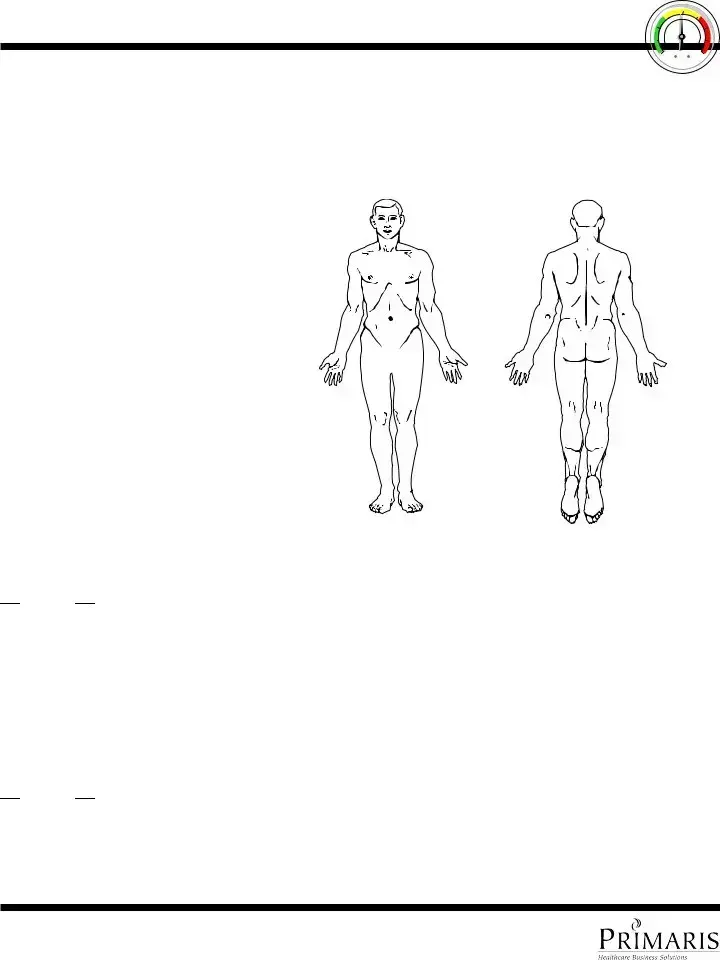
- Use the body chart included in the form to describe and graph the location of each abnormality by number.
- Sign the form in the section labeled CNA Signature: and include the date.
- Indicate whether the resident needs their toenails cut by circling Yes or No.
- Have the charge nurse sign the form in the Charge Nurse Signature: section and include the date.
- In the Charge Nurse Assessment: section, provide any additional observations or comments regarding the resident's skin condition.
- Document any interventions that were taken in the Intervention: section.
- Finally, indicate whether the issue was forwarded to the Director of Nursing (DON) by circling Yes or No.
- The DON should then sign the form in the DON Signature: section and include the date.
Document Breakdown
| Fact Name | Description |
|---|---|
| Purpose | The CNA Shower Sheets form is designed for documenting skin assessments during resident showers. |
| Skin Monitoring | CNA staff must visually assess a resident's skin and report any abnormalities to the charge nurse immediately. |
| Documentation Requirement | All findings, including the location and description of any skin abnormalities, must be recorded on the form. |
| Signature Requirement | The form requires signatures from both the CNA and the charge nurse to validate the assessment and intervention. |
| State-Specific Law | This form is governed by Missouri state regulations, particularly those related to nursing home care and resident safety. |
FAQ
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed to facilitate a thorough visual assessment of a resident's skin during showering. It helps Certified Nursing Assistants (CNAs) document any abnormalities they observe, such as bruising, rashes, or skin tears. This documentation is crucial for ensuring that any issues are reported to the charge nurse and addressed promptly, thereby maintaining the resident's skin health and overall well-being.
How should I use the body chart included in the form?
The body chart is a visual tool for CNAs to indicate the exact location of any skin abnormalities. When you notice an issue, such as a bruise or rash, mark the corresponding area on the chart with a number. In the section provided, describe the abnormality in detail. This helps ensure that the charge nurse and Director of Nursing (DON) have a clear understanding of the problem's location and nature.
What types of skin abnormalities should I look for?
During the shower, CNAs should be vigilant for a variety of skin issues, including:
- Bruising
- Skin tears
- Rashes
- Swelling
- Dryness
- Soft heels
- Lesions
- Decubitus ulcers
- Blisters
- Scratches
- Abnormal color
- Abnormal skin temperature (hot or cold)
- Hardened skin (orange peel texture)
- Any other abnormalities
Being thorough in your assessment can prevent further complications for the resident.
What should I do if I find an abnormality?
If you observe any abnormal skin condition, it is essential to report it to the charge nurse immediately. Document the findings on the form, including the specific location and description of the abnormality. The charge nurse will then assess the situation and determine the appropriate intervention, ensuring that the issue is addressed promptly.
Is there a section for documenting toenail care?
Yes, the form includes a specific question regarding whether the resident needs their toenails cut. You can indicate 'Yes' or 'No' based on your assessment. If the resident does need toenail care, this information can be communicated to the charge nurse for further action.
How do I ensure proper follow-up after reporting an abnormality?
After reporting an abnormality, it is important to ensure that the issue is forwarded to the Director of Nursing (DON) if necessary. The form provides a section for indicating whether the issue has been forwarded. Make sure to obtain the DON's signature and document the date to confirm that the issue has been addressed appropriately.
Where can I access this form?
The CNA Shower Sheets form is available online at www.primaris.org. It is important to have access to the most current version of the form to ensure compliance with best practices in resident care.
Fill out Other Forms
How to Change a Car Title - The document must include the name of the contractor and the owner of the property in question.
Cat Health Certificate - Some regions may have strict rules regarding pet vaccinations.
For anyone looking to understand the nuances of property transfer, utilizing the correct Arizona Deed form is vital for a smooth transaction. By addressing the specifics required in this document, you ensure that all necessary details are captured efficiently. For further guidance, refer to the resources available on the accurate Arizona Deed form process.
Florida State Return - Completing this form can provide peace of mind during tax season.
Cna Shower Sheets Example
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.